The rising cost of Long COVID and ME/CFS in Germany - update provides new data for 2025
An updated analysis by Risklayer and the ME/CFS Research Foundation on the prevalence and cost of Long COVID and ME/CFS in Germany provides new data for the year 2025. The report, published in April 2026, covers data for the entire six-year period between 2020 and 2025 and concludes that both illnesses continue to pose a significant burden to society. This website summarises key findings and recommendations from the report. All reports, including the first publication from May 2025 with a detailed description of the model developed to generate the novel data, can be accessed via the download links below.
What are the key findings?
In addition to causing acute illness, COVID-19 has triggered a growing wave of long-term health conditions that continue to affect millions of people, resulting in rising socio-economic costs. Aside from what is known as Long COVID or post-COVID syndrome, ME/CFS (myalgic encephalomyelitis / chronic fatigue syndrome), too, has long been suspected to cause substantial costs to society. Until now, neither the total number of people affected by both conditions, nor the extent to which the two diseases are causing damage in terms of economic, social, and medical costs to society in Germany has been known.
With an update of the first report, jointly published in May 2025 by ME/CFS Research Foundation and Risklayer, both organisations have released new data in April 2026 on the number of people living with ME/CFS or Long COVID in Germany and the costs these diseases cause.
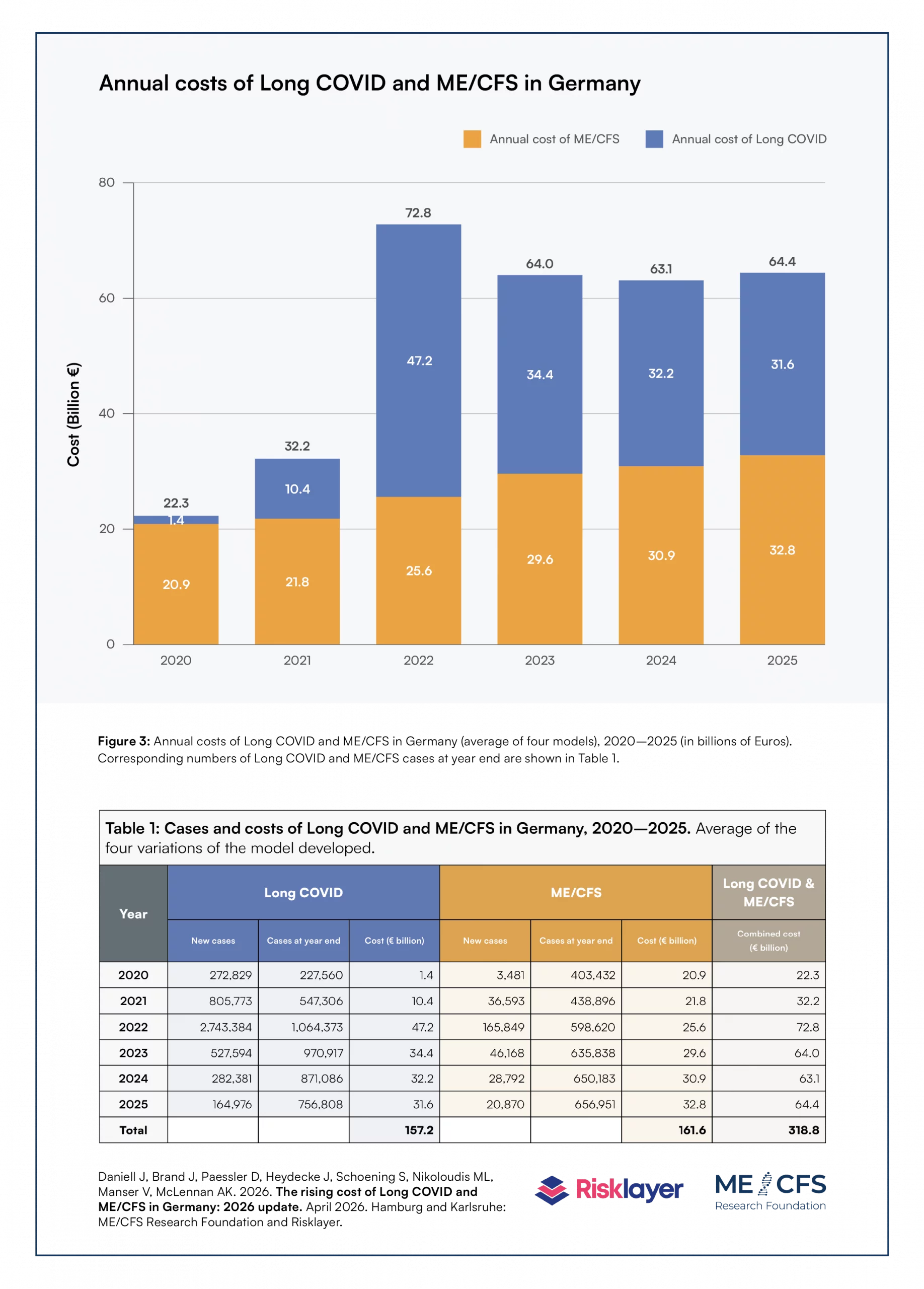
The findings of the new report point to an ongoing social burden: In the six-year period between 2020 and 2025 Long COVID and ME/CFS cost Germany €318.8 billion. In 2025 alone, Long COVID and ME/CFS cost €64.4 billion, equal to 1.44 % of Germany's gross national product (GDP) the same year. The annual costs for the entire period modelled are shown in figure 3 and table 1 of the new report.
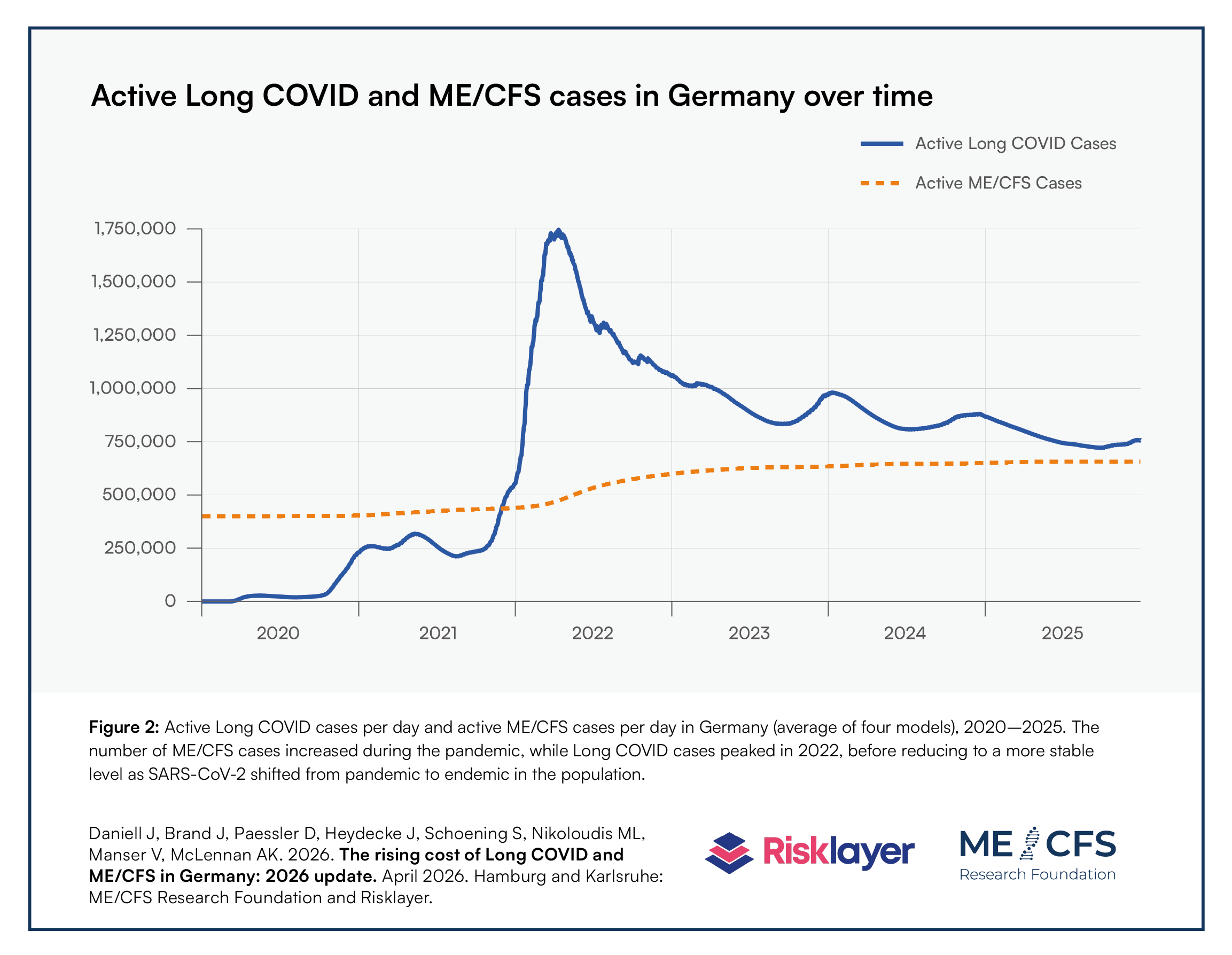
Using an innovative approach, by combing existing data and findings from literature with novel data from a model specifically developed for this report, the authors show that, at the end of 2025, 756.808 people in Germany were living with Long COVID, while an additional 656.951 people were living with ME/CFS (the latter includes ME/CFS diagnosed as a result of COVID-19/Long COVID). The numer of ME/CFS cases increased compared to the previous year, while the number of Long COVID cases slightly decreased (table 1). In total, more than 1.4 million people in Germany were living with either Long COVID or ME/CFS at the end of 2025.
Click on the image to open a detailed view and download the image in high quality.
Interview with Risklayer
Interview on the May 2025 report. Subtitles available in German and English (How do I turn on captions in YouTube videos?)
Presentation of results
Presentation of the study results at the ME/CFS Symposium 2025 - Research and Care in Germany.
Press coverage on the report
Media coverage of the report update as of April 2026 (external links):
- Der Spiegel: “ME/CFS und Long Covid kosten die Gesellschaft jährlich rund 64 Milliarden Euro”
- manager magazin: „Ein Riesenproblem mitten in der Gesellschaft“
- Tagesspiegel: „Von allein wird dieses Problem nicht verschwinden“: ME/CFS und Long Covid kosten Gesellschaft 2025 rund 64 Milliarden Euro
- Deutschlandfunk: Bildungslücken, Arbeitsausfälle, Milliardenkosten: Folgen von Post-Covid
Media coverage of the initial report as of May 2025 (external links):
- Der Spiegel (10.05.2025): “Long Covid und ME/CFS kosten die Gesellschaft jährlich 60 Milliarden Euro”
- Frankfurter Allgemeine Zeitung (FAZ) (13.05.2025): “Folgekosten der Pandemie: Der lange Arm des Virus”
- Stern (11.05.2025) “Medienbericht: Long Covid und ME/CFS kosten Gesellschaft 63 Milliarden Euro jährlich” (11.06.2025): “Long Covid und ME/CFS: Das teure Erbe der Pandemie
- manager magazin (12.05.2025): “Long Covid und ME/CFS: Das teure Erbe der Pandemie”
- Der Tagesspiegel (11.05.2025): “Studie zu Virusinfektion: Long Covid und ME/CFS kosten Gesellschaft mehr als 60 Milliarden Euro pro Jahr"
- Der Tagesspiegel (13.05.2025): “Die 60-Milliarden-Krankheit: Warum es richtig ist, die Kosten von Long Covid akribisch vorzurechnen”
- Deutsches Ärzteblatt (12.05.2025): “Die 60-Milliarden-Krankheit: Warum es richtig ist, die Kosten von Long Covid akribisch vorzurechnen”
- Frankfurter Rundschau (16.05.2025): “Erschreckende Zahlen: Long Covid kostet Deutschland etliche Milliarden pro Jahr”
- Frankfurter Allgemeine Presse (16.05.2025): “Alarmierende Statistik: Deutschland verliert jährlich Milliarden durch Long Covid”
- N-TV Nachrichten (11.05.2025): “Hunderttausende sind erkrankt: Long Covid und ME/CFS kosten 60 Milliarden Euro pro Jahr”
- Neue Züricher Zeitung (NZZ) (14.05.2025) “Long Covid und ME/CFS: Milliardenkosten belasten Deutschland”
- AOK (12.05.2025): “250 Milliarden Folgekosten durch Long Covid und ME/CFS seit 2020”
- Tagesspiegel Background (23.07.2025): “Daten als Hoffnungsträger”
- SWR Kultur (09.09.2025): “So viel kostet uns die Krankheit ME/CFS pro Jahr”
Click on the image to open a detailed view and download the image in high quality.
How does the model work?
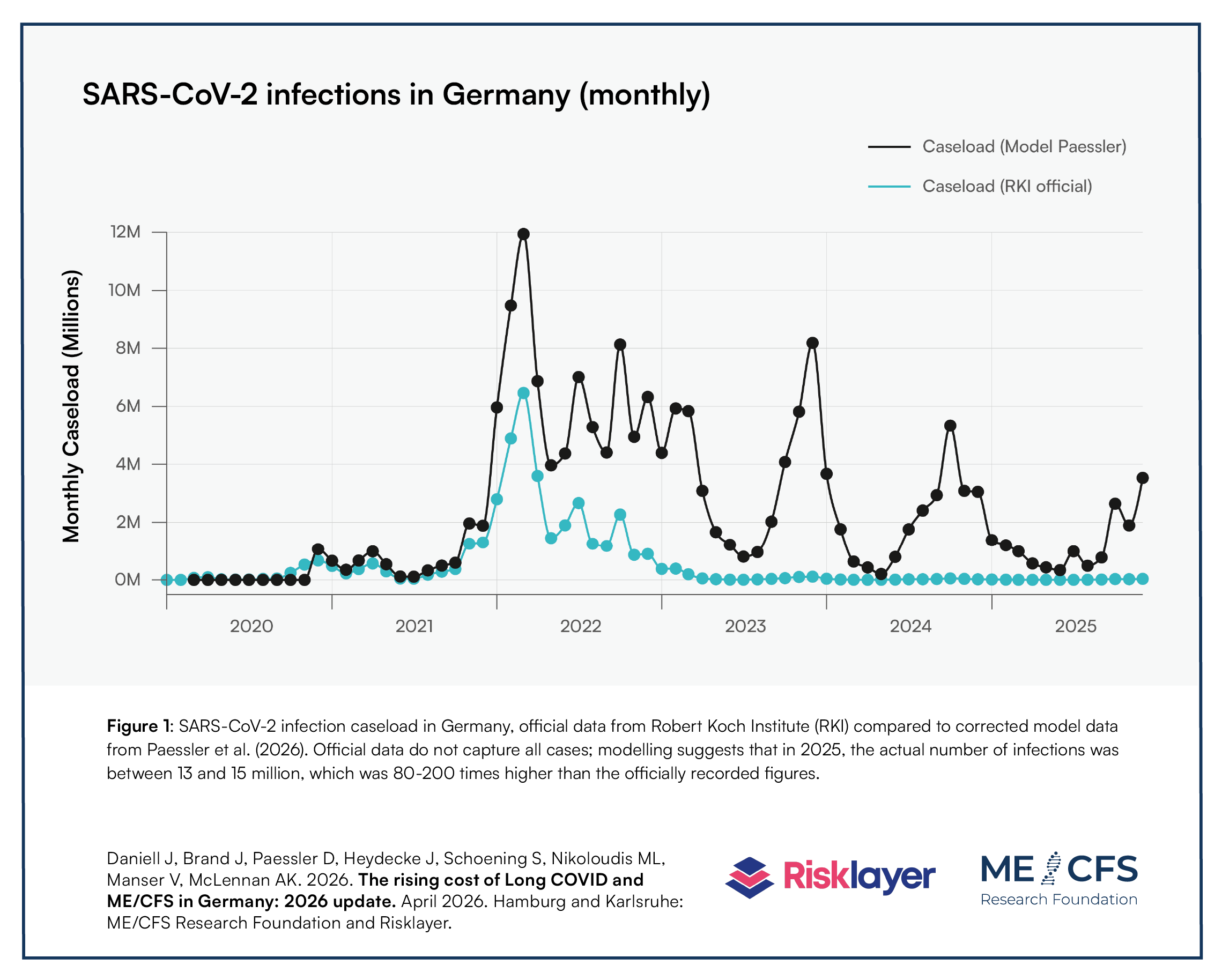
The underlying data basis for modelling the prevalence of Long COVID and ME/CFS for the purpose of this report stems from a corrected modelling of the number of monthly SARS-CoV-2 infections in Germany since the start of the COVID-19 pandemic. This alternative model is available as a preprint publication. It indicates that in 2024-2025, the number of SARS-CoV-2 infections was likely 80-200 times higher than official data by the Robert Koch Institute (the federal public health institute in Germany) suggests. This can be seen in figure 1 of the report. In 2025, the number of SARS-CoV-2 infections was therefore likely between 13 and 15 million.
Based on the corrected number of SARS-CoV-2 infections, the report's own data model, which was specifically developed by the authors, generates data on the number of active Long COVID as well as ME/CFS cases in Germany and how these developed over time. While Long COVID cases peaked in 2022, before reducing to a more stable level as SARS-CoV-2 became endemic in the population, according to the model, the number of ME/CFS cases steadily increased during the pandemic (figure 2). Indeed, a number of international experts predicted that the already comparably high number of people living with ME/CFS in the general population would likely substantially increase with the spread of SARS-CoV-2.
Click on the image to open a detailed view and download the image in high quality.

Click on the image to open a detailed view and download the image in high quality.
In order to generate data on the number of active Long COVID and ME/CFS cases over time, the report's data model makes use of both the corrected number of SARS-CoV-2 infections (see figure 1) as well as a range of existing findings from scientific literature. These findings cover assumptions on how many of the people who contract SARS-CoV-2 go on to develop Long COVID, how many of these Long COVID cases remain ill for more than a year and how many of the Long COVID cases transition to ME/CFS. The model also takes into account the share of people recovering from Long COVID and ME/CFS over time (for ME/CFS the overall recovery rate has been found to be very low, only at around 5% per year). Key assumptions and how these are fit into the model flow are depicted in figure 8 of the first report published in May 2025.
For the new analysis released in April 2026, the authors again reviewed the international literature available. Details can be found in the report. In short, based on the review, no changes were made compared to the assumptions of the original report from May 2025, meaning that the fundamental structure of the developed data model and the parameters used remain unchanged. New scientific findings may lead to a revision of the data model in the future.
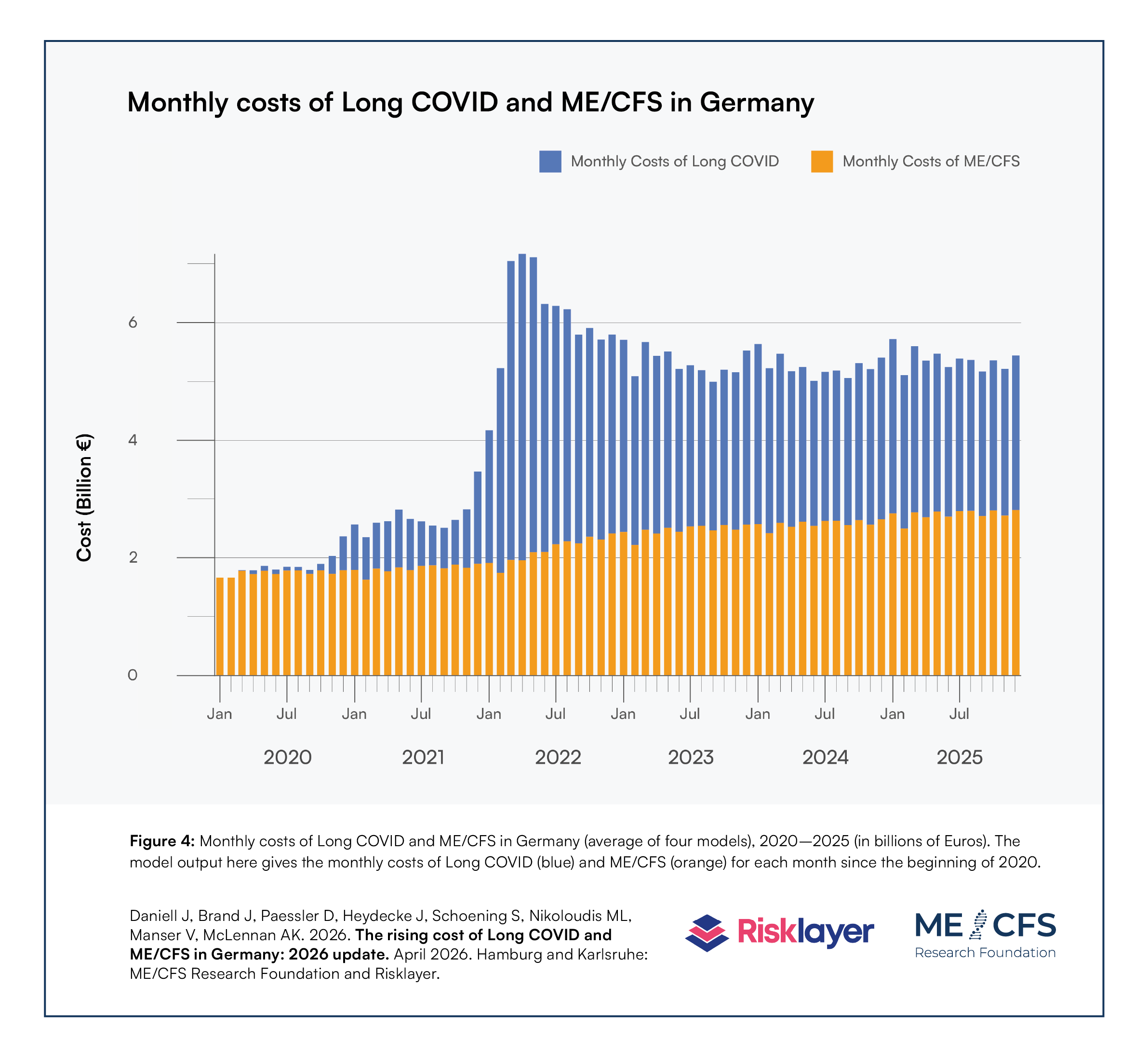
On the basis of the modelled number of Long COVID and ME/CFS cases, the model proceeds with defining the costs arising from the two diseases. These costs result from reduced value-add and increased expenditure, calculated according to standard economic parameters. Specifically, the model calculates the following costs: production disturbance costs, human capital costs, medical costs, administrative costs, travel costs, support and assistance costs, deadweight costs of transfer payments, and quality of life and well-being costs. These are then multiplied by different severity multipliers for Long COVID and ME/CFS, where a disability or severity weighting is a factor on a scale from 0 to 100% which reflects the severity of health loss associated with the particular condition, where 0 represents full health and 100% represents a full burden and not being able to work (see Annex 2 in the May 2025 report for a detailed description). The model generates monthly costs arising from Long COVID and ME/CFS over the observed period, as illustrated in figure 4 of the new report. The sum of all these costs results in the total combined cost of €318.8 billion for 2020-2025.
As can be seen in figure 4 of the report, the monthly costs of Long COVID and ME/CFS remained at a more or less stable and high level since 2022/2023. Currently, there is no reason to assume that the high level of costs is going to decrease on its own.
Click on the image to open a detailed view and download the image in high quality.
Why is this data model important?
In the absence of any reliable data on the prevalence and the costs of Long COVID and ME/CFS in Germany, it has remained difficult for stakeholders, such as the German government and, for example, the country’s pharmaceutical sector, to measure up an adequate and justified response in terms of public spending and investment in research. Up until the end of 2025, some €150 million have been allocated to health care services research by the Federal Ministry of Health (BMG), with another roughly €50 million provided for clinical and basic research by the Federal Ministry of Research, Technology and Space (BMFTR). As such, the federal government spent approximately €40 million annually on Long COVID and ME/CFS research during the five-year period up until the end of 2025. Compared to the combined cost of both diseases in Germany in 2025 of €64.4 billion, average annual spending on research by the federal government equaled 0.06%. Some state governments, too, have made funds available for dedicated research projects. However, a coordinated, nationwide research strategy has yet to be implemented.
Some efforts by the federal government of Germany are underway to address the current evidence gap on prevalence and costs. Such efforts include the Federal Joint Committee (G-BA)-funded project BD-LC-PS and the BMG-funded projects MultiCARE and HELoCO.Results or even preliminary data from these projects are expected earliest at the end of 2026 and more likely in 2027 and beyond.
With any official data unlikely to be available soon, ME/CFS Research Foundation and Risklayer felt that it was important to provide new – and in the eyes of the authors currently still the most up-to-date and complete – estimates on the prevalence and cost of Long COVID and ME/CFS in Germany. With the release of the April 2026 update, both organisations intend to continue to inform wide-ranging discussions about how best to shape public policy, funding, research, and health systems to improve overall outcomes and reduce costs for people living with Long COVID and ME/CFS, communities, governments and society at large.
What are the recommendations?
German state and federal governments have been proactive in raising awareness and improving the overall care situation for people living with Long COVID and ME/CFS, as well as providing funding for basic, clinical and epidemiological research.
The end of 2025 saw the announcement of the "National Decade Against Post-infectious Diseases" (external link). Equipped with a total of €500 million over a period of 10 years, with it the German Federal Government has now announced an ambitious research programme. As part of the "National Decade", €50 million will be spent annually on research into post-infectious diseases. The goal is to better understand the underlying mechanisms of illnesses such as Long COVID and ME/CFS, to be able to develop targeted therapies. The latest report from Risklayer and ME/CFS Research Foundation contains concrete policy recommendations on how funding under the “National Decade” could be used to achieve a rapid and sustainable reduction in the modeled societal cost. The authors emphasise that the overarching goal must be to develop safe and effective therapies as soon as possible and make them available to all patients nationwide. Only in this way can an effective reduction of the considerable societal cost be achieved. These and other recommendations are detailed in the final chapter of the April 2026 report.
1. Invest in biomarkers, diagnostics, and treatments
In the absence of any reliable data on the prevalence and the costs of Long COVID and ME/CFS in Germany, it has remained difficult for stakeholders, such as the German government and, for example, the country’s pharmaceutical sector, to measure up an adequate and justified response in terms of public spending and investment in research. Up until the end of 2025, some €150 million have been allocated to health care services research by the Federal Ministry of Health (BMG), with another roughly €50 million provided for clinical and basic research by the Federal Ministry of Research, Technology and Space (BMFTR). As such, the federal government spent approximately €40 million annually on Long COVID and ME/CFS research during the five-year period up until the end of 2025. Compared to the combined cost of both diseases in Germany in 2025 of €64.4 billion, average annual spending on research by the federal government equaled 0.06%. Some state governments, too, have made funds available for dedicated research projects. However, a coordinated, nationwide research strategy has yet to be implemented.
Some efforts by the federal government of Germany are underway to address the current evidence gap on prevalence and costs. Such efforts include the Federal Joint Committee (G-BA)-funded project BD-LC-PS and the BMG-funded projects MultiCARE and HELoCO.Results or even preliminary data from these projects are expected earliest at the end of 2026 and more likely in 2027 and beyond.
With any official data unlikely to be available soon, ME/CFS Research Foundation and Risklayer felt that it was important to provide new – and in the eyes of the authors currently still the most up-to-date and complete – estimates on the prevalence and cost of Long COVID and ME/CFS in Germany. With the release of the April 2026 update, both organisations intend to continue to inform wide-ranging discussions about how best to shape public policy, funding, research, and health systems to improve overall outcomes and reduce costs for people living with Long COVID and ME/CFS, communities, governments and society at large.
2. Close the biomedical funding gap
Until the end of 2025, research on biomarkers, diagnostics, and treatments had accounted for only 22% (€50 million) of the cumulative total €221 million in funding allocated to ME/CFS and Long COVID research by the Federal Government of Germany since 2022. No more than 18% (€35–40 million) of this funding to date has been allocated to biomedical ME/CFS research. In contrast, approximately €157 million (or 71%) of all federal research funding for these diseases to date has been directed toward healthcare services research, including measures such as rehabilitation and psychotherapy. While the latter interventions assist some patients in managing their illness, they do not change the disease state, especially in people living with ME/CFS and Long COVID characterised by post-exertional malaise (PEM), and are thereby unlikely to reduce the societal costs reported here.
The model points to key leverage points for reducing the cost of Long COVID and ME/CFS around finding effective treatments and improving diagnostics (and so improving data and tailored care), alongside reducing infection rates (detailed in the May 2025 report). Closing the significant biomedical funding gap around these conditions in and through the "National Decade" agenda is therefore key to reducing costs and improving outcomes. This could include: (a) prioritising research on identifying pathophysiological disease mechanisms and establishing reliable diagnostics, with the aim of defining disease phenotypes and stratifying patient subgroups; (b) fast-tracking the development of viable pharmacological treatment options by trialing the repurposing of existing drugs and development of novel compounds; and, (c) inviting emerging fields of biomedicine to innovate in this area.
3. Accelerate research through learning and feedback loops
The The present results reinforce how time-critical change is in the area of Long COVID and ME/CFS, with costs continuing to mount even as new policy and funding is developed and deployed. One way the "National Decade" can expedite change is to support research infrastructures and networks of expertise in Germany – where expertise includes patient experts and managers alongside scientists and healthcare practitioners – to accelerate in parallel the generation, validation, implementation and scaling of already existing and still-to-be-generated evidence from Long COVID and ME/CFS research. One guiding principle must be to maximise the efficiency and speed with which effective therapies can be made available to patients, alongside safety and accessibility.
This could be achieved, for example, by (a) rolling out basic, translational, and clinical research (including in the form of drug trials) at an early stage at the same time, (b) using existing infrastructure such as adaptive platform trials, (c) enhancing feedback loops through collective work, and (d) enabling the participation of regulators, the private sector and industry. When it comes to creating, awarding and administering research funding, lessons from past shortcomings should be acknowledged and addressed in future. Research commissioning should include clear guidelines on disease definitions, diagnostic and inclusion criteria, with incentives for sharing lessons learned. Studies with overly broad inclusion criteria or insufficient emphasis on subgroup analyses which have often resulted in diluted findings should be avoided. There are also opportunities for efficiency in harmonising studies and trials to ensure the timely and efficient use of resources and comparability of results.
4. Incentivise collaboration and open science
The successful development of the model presented here is underpinned by bringing together diverse types of expertise to deliver a research outcome that is open to public sharing and scrutiny. Such collaboration and openness can lead to greater pace, innovation and real-world impact of research, without compromising quality. For this reason, another guiding principle that would benefit the "National Decade" is to incentivise open data and collaboration rather than competitiveness at all stages of delivery.
The "National Decade" should continue to build on the accumulated evidence and knowledge from ME/CFS and Long COVID research in Germany and internationally – both published and in the form of experience. Bringing together medical practitioners with direct experience in diagnosing and/or treating these diseases, patient experts and people with lived experience, in all stages of the work – from strategic decision making to designing calls for funding, reviewing funding proposals to implementing research – will ensure Germany capitalises on the landscape of expertise it has already fostered, and which sits behind the "National Decade".
5. Improve data collection
In the April 2026 update, the model continues to point to the importance of reducing the overall SARS-CoV-2 infection load throughout the population. Recommendations relating to public health measures on preventing the spread of infections (see May 2025 report), including improving air quality, are still relevant here. In addition, there is a need to maintain existing and build improved data collection infrastructure for infectious diseases (e.g. by continuing RKI’s AMELAG wastewater virus monitoring). Improved disease surveillance will be necessary to better identify hotspots for targeted public health interventions, at-risk groups, and to ultimately monitor and evaluate the effectiveness of the "National Decade" in the longer-term.
While the present model continues to be key to informing decision-making around post-infectious diseases in Germany, eventually good real-world data should replace the need for stochastic modelling. The work of data collection to this end is beyond the scope of the "National Decade", which underscores the importance of cross-agency collaboration and additional investment to improve outcomes and reduce costs around Long COVID and ME/CFS in Germany.
Download full reports
Download full reports
Why is this data model important?
In the absence of any reliable data on the prevalence and the costs of Long COVID and ME/CFS in Germany, it has remained difficult for stakeholders, such as the German government and, for example, the country’s pharmaceutical sector, to measure up an adequate and justified response in terms of public spending and investment in research. Up until the end of 2025, some €150 million have been allocated to health care services research by the Federal Ministry of Health (BMG), with another roughly €50 million provided for clinical and basic research by the Federal Ministry of Research, Technology and Space (BMFTR). As such, the federal government spent approximately €40 million annually on Long COVID and ME/CFS research during the five-year period up until the end of 2025. Compared to the combined cost of both diseases in Germany in 2025 of €64.4 billion, average annual spending on research by the federal government equaled 0.06%. Some state governments, too, have made funds available for dedicated research projects. However, a coordinated, nationwide research strategy has yet to be implemented.
Some efforts by the federal government of Germany are underway to address the current evidence gap on prevalence and costs. Such efforts include the Federal Joint Committee (G-BA)-funded project BD-LC-PS and the BMG-funded projects MultiCARE and HELoCO.Results or even preliminary data from these projects are expected earliest at the end of 2026 and more likely in 2027 and beyond.
With any official data unlikely to be available soon, ME/CFS Research Foundation and Risklayer felt that it was important to provide new – and in the eyes of the authors currently still the most up-to-date and complete – estimates on the prevalence and cost of Long COVID and ME/CFS in Germany. With the release of the April 2026 update, both organisations intend to continue to inform wide-ranging discussions about how best to shape public policy, funding, research, and health systems to improve overall outcomes and reduce costs for people living with Long COVID and ME/CFS, communities, governments and society at large.
What are the recommendations?
German state and federal governments have been proactive in raising awareness and improving the overall care situation for people living with Long COVID and ME/CFS, as well as providing funding for basic, clinical and epidemiological research.
The end of 2025 saw the announcement of the "National Decade Against Post-infectious Diseases" (external link). Equipped with a total of €500 million over a period of 10 years, with it the German Federal Government has now announced an ambitious research programme. As part of the "National Decade", €50 million will be spent annually on research into post-infectious diseases. The goal is to better understand the underlying mechanisms of illnesses such as Long COVID and ME/CFS, to be able to develop targeted therapies. The latest report from Risklayer and ME/CFS Research Foundation contains concrete policy recommendations on how funding under the “National Decade” could be used to achieve a rapid and sustainable reduction in the modeled societal cost. The authors emphasise that the overarching goal must be to develop safe and effective therapies as soon as possible and make them available to all patients nationwide. Only in this way can an effective reduction of the considerable societal cost be achieved. These and other recommendations are detailed in the final chapter of the April 2026 report.
1. Invest in biomarkers, diagnostics, and treatments
According to the model, one of the main factors driving the societal cost of Long COVID and ME/CFS in Germany is the low rate of recovery from these diseases, ME/CFS in particular. This points to a major opportunity space around clinically-relevant research.
Targeted investments under the "National Decade" prioritising the rapid development of safe, effective, and widely-available treatments would drive down costs and significantly improve the lives of people living with post-infectious diseases. Early investments in treatment development would also lay the foundation for longer-term basic research to understand disease mechanisms. It requires government to both invest in research on biomarkers, diagnostics and therapies, and establish clear incentives and requirements around safety, access and open science.
There is also work to be done to improve patient outcomes, advance science and drive down the costs calculated in this model which is beyond the scope of the "National Decade". Simultaneously laying the foundations for a rapid path to translation and implementation with and through other government departments and organisations is of key importance.
2. Close the biomedical funding gap
Until the end of 2025, research on biomarkers, diagnostics, and treatments had accounted for only 22% (€50 million) of the cumulative total €221 million in funding allocated to ME/CFS and Long COVID research by the Federal Government of Germany since 2022. No more than 18% (€35–40 million) of this funding to date has been allocated to biomedical ME/CFS research. In contrast, approximately €157 million (or 71%) of all federal research funding for these diseases to date has been directed toward healthcare services research, including measures such as rehabilitation and psychotherapy. While the latter interventions assist some patients in managing their illness, they do not change the disease state, especially in people living with ME/CFS and Long COVID characterised by post-exertional malaise (PEM), and are thereby unlikely to reduce the societal costs reported here.
The model points to key leverage points for reducing the cost of Long COVID and ME/CFS around finding effective treatments and improving diagnostics (and so improving data and tailored care), alongside reducing infection rates (detailed in the May 2025 report). Closing the significant biomedical funding gap around these conditions in and through the "National Decade" agenda is therefore key to reducing costs and improving outcomes. This could include: (a) prioritising research on identifying pathophysiological disease mechanisms and establishing reliable diagnostics, with the aim of defining disease phenotypes and stratifying patient subgroups; (b) fast-tracking the development of viable pharmacological treatment options by trialing the repurposing of existing drugs and development of novel compounds; and, (c) inviting emerging fields of biomedicine to innovate in this area.
3. Accelerate research through learning and feedback loops
The The present results reinforce how time-critical change is in the area of Long COVID and ME/CFS, with costs continuing to mount even as new policy and funding is developed and deployed. One way the "National Decade" can expedite change is to support research infrastructures and networks of expertise in Germany – where expertise includes patient experts and managers alongside scientists and healthcare practitioners – to accelerate in parallel the generation, validation, implementation and scaling of already existing and still-to-be-generated evidence from Long COVID and ME/CFS research. One guiding principle must be to maximise the efficiency and speed with which effective therapies can be made available to patients, alongside safety and accessibility.
This could be achieved, for example, by (a) rolling out basic, translational, and clinical research (including in the form of drug trials) at an early stage at the same time, (b) using existing infrastructure such as adaptive platform trials, (c) enhancing feedback loops through collective work, and (d) enabling the participation of regulators, the private sector and industry. When it comes to creating, awarding and administering research funding, lessons from past shortcomings should be acknowledged and addressed in future. Research commissioning should include clear guidelines on disease definitions, diagnostic and inclusion criteria, with incentives for sharing lessons learned. Studies with overly broad inclusion criteria or insufficient emphasis on subgroup analyses which have often resulted in diluted findings should be avoided. There are also opportunities for efficiency in harmonising studies and trials to ensure the timely and efficient use of resources and comparability of results.
4. Incentivise collaboration and open science
The successful development of the model presented here is underpinned by bringing together diverse types of expertise to deliver a research outcome that is open to public sharing and scrutiny. Such collaboration and openness can lead to greater pace, innovation and real-world impact of research, without compromising quality. For this reason, another guiding principle that would benefit the "National Decade" is to incentivise open data and collaboration rather than competitiveness at all stages of delivery.
The "National Decade" should continue to build on the accumulated evidence and knowledge from ME/CFS and Long COVID research in Germany and internationally – both published and in the form of experience. Bringing together medical practitioners with direct experience in diagnosing and/or treating these diseases, patient experts and people with lived experience, in all stages of the work – from strategic decision making to designing calls for funding, reviewing funding proposals to implementing research – will ensure Germany capitalises on the landscape of expertise it has already fostered, and which sits behind the "National Decade".
5. Improve data collection
In the April 2026 update, the model continues to point to the importance of reducing the overall SARS-CoV-2 infection load throughout the population. Recommendations relating to public health measures on preventing the spread of infections (see May 2025 report), including improving air quality, are still relevant here. In addition, there is a need to maintain existing and build improved data collection infrastructure for infectious diseases (e.g. by continuing RKI’s AMELAG wastewater virus monitoring). Improved disease surveillance will be necessary to better identify hotspots for targeted public health interventions, at-risk groups, and to ultimately monitor and evaluate the effectiveness of the "National Decade" in the longer-term.
While the present model continues to be key to informing decision-making around post-infectious diseases in Germany, eventually good real-world data should replace the need for stochastic modelling. The work of data collection to this end is beyond the scope of the "National Decade", which underscores the importance of cross-agency collaboration and additional investment to improve outcomes and reduce costs around Long COVID and ME/CFS in Germany.
What are the limitations of the report?
Limitations of the report and its data model relate first and foremost to the general lack of data. This includes a lack of infection surveillance (such as cases of COVID-19 overall, Long COVID and ME/CFS incidence and prevalence, fluctuation of non-COVID-19-related ME/CFS cases during the various stages of the pandemic and related public health measures, data on recovery rates for both Long COVID and ME/CFS), as well as lack of long-term data due to the relative newness of Long COVID.
This means there is insufficient longitudinal data to understand completely the effects of vaccination, infection-derived immunity, different virus strains, geographical location, or other factors on disease progression and resolution. Where necessary, assumptions were made in the model about these based on the best available secondary data. Limitations also relate to biased data. Where the model draws on secondary data, such as employer and health insurer data, a number of biases might be present.
Noteworthy, among other things, the model assumes that non-COVID-19-related ME/CFS case numbers remained constant over time, with only COVID-19-related ME/CFS having increased since 2020. This means the modelled number of ME/CFS cases is likely an underestimation.
Another limitation of the model used in the report is its use of the so-called Monte Carlo simulation, which is computationally intensive and require significant expertise to carry out. This type of simulation cannot easily be re-run, explained for non-specialists to understand, or replicated by all reviewers for complete verification. Annex 2 of the May 2025 report aims to provide sufficient details on this modelling approach. The model data is also provided on GitHub, .
The report provides an overview of other, existing studies which have taken similar approaches at estimating and modelling the different costs of Long COVID and ME/CFS (Tables 2 and 3 in Annex 1 of the May 2025 report). That the model’s various findings broadly align with research published by others lends further weight to its reliability. Generally, the report’s authors concluded that the model’s findings are conservative and more likely to underestimate rather than overestimate costs.
Who are the authors?
Die datenbasierte Modellierung in den bisher zwei veröffentlichten Berichten wurde von den Risikomanagement-Experten der Risklayer GmbH. Risklayer has been providing risk analytics and risk management to governments all over the world since 2014. For the initial years of the COVID-19 pandemic, Risklayer maintained a detailed day-by-day SARS-CoV-2 infections caseload dataset for all 401 districts in Germany, based in part on a novel crowdsourcing approach for data. The comprehensive data provided by Risklayer was utilized and frequently cited by major German media outlets and as the basis for official counting of cases and trends in Germany through the first two years of the pandemic.
Through this practical experience, Risklayer has cultivated extensive expertise in COVID-19 caseload data within Germany. This proficiency is augmented by Risklayer's ongoing practice of modelling the consequences of critical events and natural disasters, from seismic activity and severe meteorological occurrences to conflict. The reliability of Risklayer's models is evidenced by their daily use by numerous governments and non-governmental organisations globally. Risklayer originated from the Center for Disaster Management and Risk Reduction Technology (CEDIM) at the Karlsruhe Institute of Technology (KIT) in Germany, and the General Sir John Monash Foundation in Australia.
The ME/CFS Research Foundation provided input on the assumptions used in the model, as well as literature reviews and engagement with networks of experts. As a non-profit organisation based in Germany, and with an international scientific advisory board, the Foundation funds biomedical research, enables the networking of researchers and experts in the field, and informs patients and the public about the status quo of research relating to both ME/CFS and subtypes of Long COVID.